Why intermediate-risk men are the right group to image
Standard cardiovascular risk calculators (Framingham, ASCVD, SCORE2) use age, sex, blood pressure, cholesterol, smoking and diabetes to produce a probability of an event in the next ten years. They work reasonably well at the extremes - someone clearly low-risk usually is, someone clearly high-risk usually is - but the majority of middle-aged men land in an intermediate band where the calculator alone cannot tell you whether to start a statin, how tightly to drive LDL, or whether to consider aspirin.
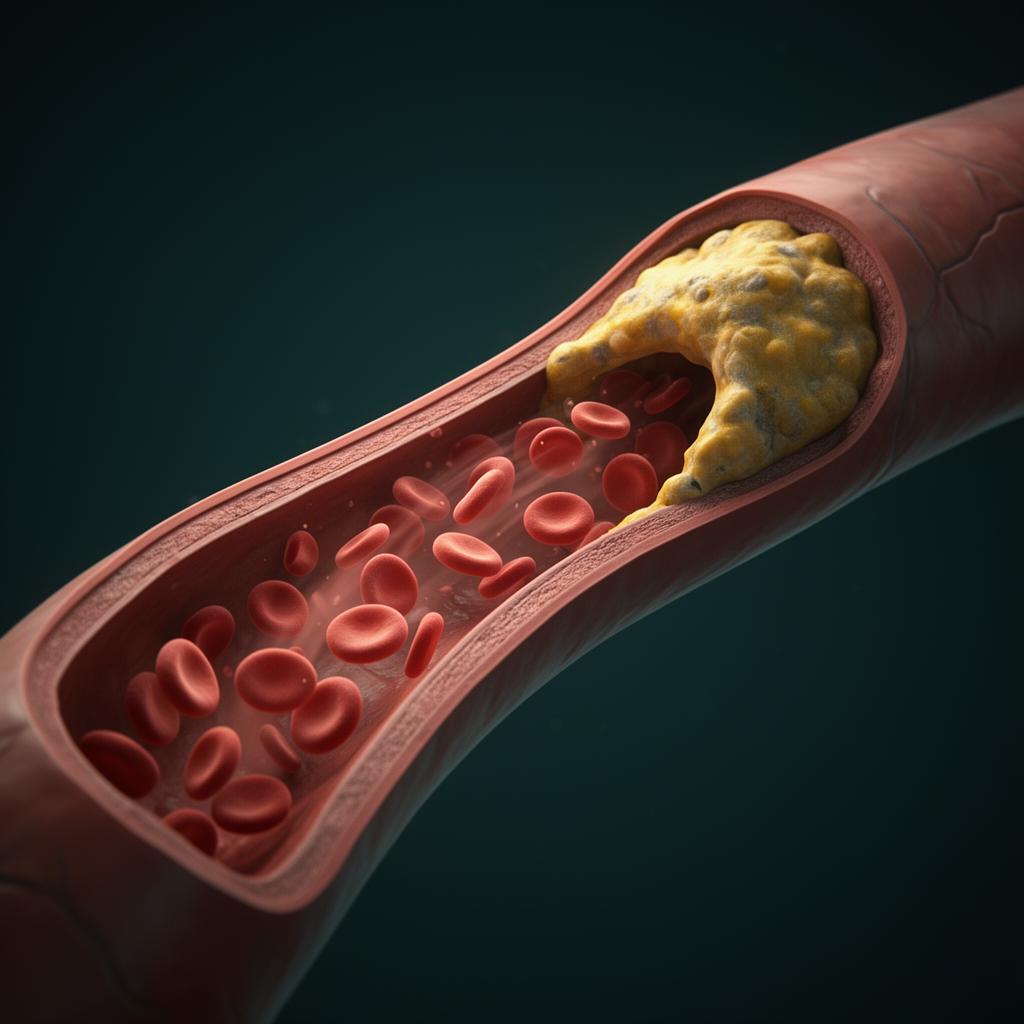
CT coronary imaging cuts through this ambiguity by showing the disease itself, not a statistical estimate. Plaque is either present in your arteries or it is not. That binary, plus the quantitative score, reclassifies a large share of intermediate-risk men: roughly half are moved down (low burden, defer therapy, recheck in years) and a meaningful minority are moved up (significant burden, start treatment earlier and more aggressively than the calculator suggested).
This is the key shift in modern preventive cardiology: stop treating averages, start treating the individual artery.